Dr. Chris Irwin
The Skin Doctor
Being diagnosed with melanoma can be scary, but the good news is that the type of melanoma you have, even though it is invasive, is still early-stage and will most likely be completely cured by simple surgical removal with margins. This handout explains thinly invasive melanoma —and why it usually does not require additional tests like lymph node biopsies or body scans. We’ll also discuss what to expect next and how these early melanomas are managed in a patient-friendly way.
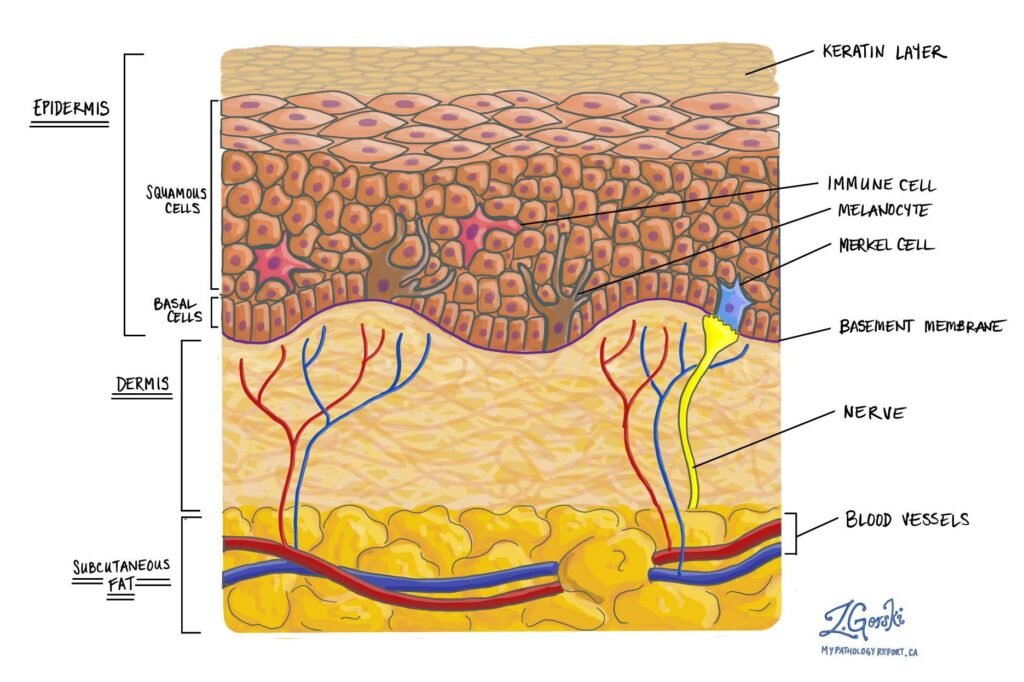
Figure 1. Histological diagram of an invasive melanoma
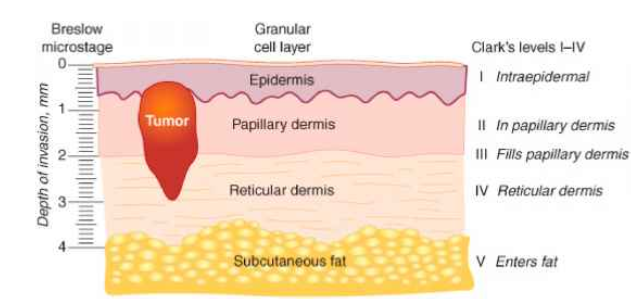
Figure 2. Explanation of Breslow thickness (credit : Steven Chen
If your report says you have an invasive melanoma with a Breslow thickness < 1mm, this is often called a “thinly invasive melanoma” and corresponds to an early Stage I melanoma. “Invasive” simply means the melanoma did grow deeper than the epidermis into the second layer of skin (dermis) – breaking through the strong canvas layer called the basement membrane or “dermo-epidermal junction”, but in this case only slightly.
Thinly invasive melanoma is more serious than in situ melanoma because there is a low chance of spread through the body. How serious an invasive melanoma is depends on several variables. The primary “badness” marker is the breslow thickness.
Breslow thickness is a measurement in millimetres from the top of the skin (technically the granular layer of the epidermis) to the deepest point of invasion by the melanoma. Let’s put this into perspective though, 1mm is the same thickness as a grain of sand. If you have a melanoma less thick than a grain of sand, the most likely outcome if you are treated properly is that everything will be completely fine.
Figure 2. Explanation of Breslow thickness (credit : Steven Chen https://x.com/DrStevenTChen/status/1345490623822921728)
The reason why we care the most about the Breslow thickness is it is the main marker for how likely a melanoma has spread to regional lymph nodes (like in the armpits or groin) – or further.
In general the risks for spread for a thinly invasive melanoma are really low – less than 5%.
Other risk factors (that will be on the histology report from the lab) that make spread more likely are:
Histology reports are very complicated and have a whole bunch of other words on them. If you have any questions about the specific words feel free to ask during your consult. In the vast majority of cases though, anything other than the breslow thickness, and the other risk factors discussed above doesn’t really alter management.
Do I need further scans or tests to make sure it hasn’t spread?
In general, no. For most patients with thinly invasive melanoma, the risks of the scans or tests outweigh the benefit they provide.
Current guidelines in Australia state that If a melanoma has a breslow thickness 0.7mm-1mm AND has any of the risk factors above (ulceration, mitotic rate >1, Clark level IV or V or Lymphovascular invasion), we discuss the role of Sentinel Lymph Node Biopsy (SLNB). (https://melanoma.org.au/wp-content/uploads/2021/11/Clinical-Brochure-Sentinal-Node-Biopsy.pdf)
In basic terms a SLNB is a procedure to see whether the closest lymph node contains any melanoma cells that have spread from the skin. It requires a general anaesthetic (being put to sleep) and has some significant risks associated with it. The overall risk of a complication from SLNB is around 11.3% (https://cinj.org/sites/cinj/files/documents/Complications%20of%20sentinel%20lymph%20node%20biopsy%20for%20melanoma%20-%20a%20systematic%20review%20of%20the%20literature.pdf). While it is important to consider this procedure if your risk of spread is >5%, we don’t recommend this procedure for most low risk thinly invasive melanomas, as we are more likely to harm you than help you with the procedure.
Key facts about thinly invasive melanomas:
Takeaway: Thin invasive melanomas (<1mm) are early-stage skin cancers with a very low risk of spread. Treatment is minor surgery to remove it with a margin. Additional procedures like lymph node biopsy or body scans are usually not done because they are not likely to find anything in such low-risk cases
Your prognosis is extremely good. Both melanoma in situ and thin invasive melanomas have high cure rates after proper removal – meaning the vast majority of patients remain alive and well, with no recurrence of melanoma. Many experts would say you are likely cured at this point. Here’s what to expect moving forward and some tips for peace of mind: